Sleep Apnea Nexus Letters

Sleep Apnea Secondary to COPD VA Claim
Many veterans with obstructive sleep apnea, also called OSA, are already service-connected for a respiratory condition such as COPD, chronic bronchitis, emphysema, asthma, asthma-COPD overlap, chronic respiratory impairment, or restrictive lung disease.
If that sounds like your situation, you may be wondering whether your sleep apnea can be claimed as secondary to COPD or another service-connected pulmonary condition.
Veterans often ask questions such as:
- Can COPD cause sleep apnea?
- Can chronic bronchitis aggravate obstructive sleep apnea?
- What is COPD–OSA overlap syndrome?
- Can chronic bronchitis, emphysema, or asthma be connected to sleep apnea?
- What if the VA says my sleep apnea is only due to obesity?
- Do I need a nexus letter for sleep apnea secondary to COPD?
The answer is that COPD and OSA can coexist in a medically recognized pattern. When both conditions are present, a veteran may experience more severe nighttime oxygen drops, disrupted sleep, daytime fatigue, reduced stamina, and greater cardiopulmonary strain than would be expected from either condition alone.
However, the VA does not usually grant secondary service connection simply because a veteran has both COPD and sleep apnea. The claim typically needs a clear medical explanation showing how the service-connected respiratory condition caused, contributed to, or aggravated the veteran’s obstructive sleep apnea.
That is where a professionally written sleep apnea nexus letter can be important. Dr. Jessica Allen prepares physician-written nexus letters for veterans seeking to claim obstructive sleep apnea secondary to COPD and related respiratory conditions. Her letters are based on the veteran’s medical records, sleep study findings, respiratory history, pulmonary symptoms, medication profile, weight history, CPAP or BiPAP use, oxygenation issues, and any prior VA denial rationale.
What Does “OSA Secondary to COPD” Mean?
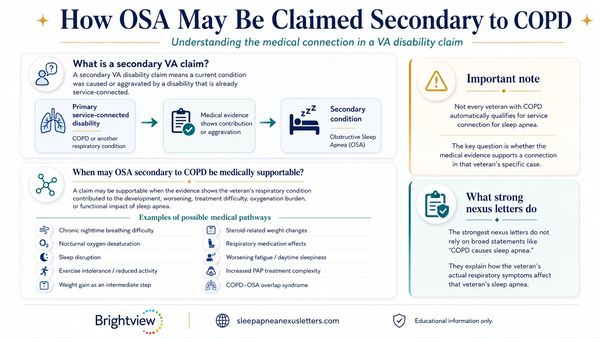
A secondary VA disability claim means that a current medical condition was caused or aggravated by a disability that is already service-connected. In this type of claim, COPD or another service-connected respiratory condition is the primary disability, and obstructive sleep apnea is the secondary condition.
A claim for OSA secondary to COPD may be medically supportable when the evidence shows that the veteran’s respiratory condition contributed to the development, worsening, treatment difficulty, oxygenation burden, or functional impact of sleep apnea. However, this does not mean that every veteran with COPD automatically qualifies for service connection for sleep apnea. The key issue is whether the medical evidence supports a connection in that veteran’s specific case.
In a sleep apnea nexus letter, Dr. Allen reviews the veteran’s respiratory history, sleep study findings, treatment records, medication history, weight history, symptoms, and prior VA rationale when applicable. She then evaluates whether the records support a medically reasoned relationship between the veteran’s service-connected respiratory condition and obstructive sleep apnea.
This analysis may involve questions such as whether COPD or a related respiratory condition affected the veteran’s nighttime breathing, oxygenation, sleep quality, daytime fatigue, treatment needs, or overall respiratory burden. When relevant, Dr. Allen may also address whether other documented factors, such as respiratory medications, activity limitations, weight changes, or COPD–OSA overlap syndrome, play a role in the veteran’s case.
The strongest nexus letters do not rely on broad statements such as “COPD causes sleep apnea.” Instead, they explain how the veteran’s actual medical history, respiratory symptoms, treatment course, and objective records support—or do not support—a medically sound connection between the service-connected respiratory condition and obstructive sleep apnea.

What Is COPD–OSA Overlap Syndrome?
COPD–OSA overlap syndrome refers to the coexistence of chronic obstructive pulmonary disease and obstructive sleep apnea in the same person.
COPD affects the lower airways and lungs. It can cause airflow limitation, impaired gas exchange, chronic cough, wheezing, shortness of breath, and reduced exercise tolerance.
OSA affects breathing during sleep. It occurs when the upper airway repeatedly collapses or becomes obstructed, causing pauses in breathing, oxygen drops, sleep fragmentation, and daytime symptoms such as fatigue or hypersomnolence.
When COPD and OSA occur together, the conditions can interact during sleep. COPD may already limit oxygen exchange, while OSA adds repeated episodes of airway obstruction and intermittent oxygen desaturation. Together, these conditions may create a heavier nighttime respiratory burden.
For a VA claim, overlap syndrome may be important because it helps explain why COPD and sleep apnea should not always be treated as completely unrelated conditions. Even if COPD did not directly create the mechanical upper airway collapse seen in OSA, COPD may still worsen the severity, symptoms, oxygenation burden, treatment complexity, or functional effects of sleep apnea.
About Respiratory System VA Ratings

Why a Secondary OSA Claim Can Matter Even When COPD Is Already Rated
The VA generally does not assign separate ratings for every coexisting respiratory condition when the conditions fall under certain respiratory diagnostic codes. Under 38 C.F.R. § 4.96, the VA applies special rules for rating coexisting respiratory conditions and generally assigns a single evaluation under the predominant disability, with elevation to the next higher evaluation when warranted by the overall severity.
Sleep apnea is rated under 38 C.F.R. § 4.97, Diagnostic Code 6847. The rating criteria include documented sleep-disordered breathing, persistent daytime hypersomnolence, use of a breathing assistance device such as CPAP, and more severe complications such as chronic respiratory failure, cor pulmonale, or tracheostomy.
This is why a secondary OSA claim may still matter.
For example, if a veteran has service-connected COPD rated below 50 percent and also has OSA requiring CPAP, the OSA evidence may be important because the VA may consider the overall respiratory disability picture under the applicable rating rules.
Essentially, if the COPD (bronchitis or emphysema) rating is 30% or less, getting a sleep apnea rating will result in an overall higher rating of 50% in most cases.
Nexus Letters Are a Financial Investment

Sleep Apnea Nexus Letters

What If the VA Blames Obesity?
The VA frequently denies sleep apnea claims by attributing OSA to obesity, body habitus, age, male sex, or airway anatomy.
Obesity is a well-known risk factor for obstructive sleep apnea. However, that does not automatically defeat a secondary service connection claim.
In some cases, obesity may be part of the medical pathway between a service-connected respiratory condition and OSA. For example, COPD may cause:
- Shortness of breath with exertion.
- Reduced stamina.
- Exercise intolerance.
- Chronic fatigue.
- Activity restriction.
- Repeated exacerbations.
- Steroid exposure.
- Weight gain over time.
That weight gain may then contribute to the development or worsening of obstructive sleep apnea.
This is sometimes referred to as obesity as an intermediate step. The argument is not simply that the veteran is obese. The argument is that the service-connected respiratory condition contributed to weight gain, and that weight gain contributed to OSA.
A strong sleep apnea nexus letter should not ignore obesity. It should explain whether obesity appears to be an unrelated risk factor, a partial contributor, or a medically relevant intermediate step connected to the service-connected disability.
Other Respiratory Conditions That May Be Relevant to a Sleep Apnea Claim
A veteran’s claim may involve COPD alone, or it may involve several related respiratory diagnoses.
Dr. Allen can evaluate whether sleep apnea is medically connected to service-connected conditions such as:
- Chronic bronchitis.
- Emphysema.
- Asthma.
- Asthma-COPD overlap.
- Restrictive lung disease.
- Chronic sinusitis.
- Allergic rhinitis.
- Deviated septum.
- Medication-related respiratory or weight effects.
- Steroid-associated weight gain.
When these conditions are documented and medically relevant, they may help explain the veteran’s full respiratory disability picture. The key is to connect the medical evidence to the specific veteran’s records.
Evidence That May Help Support an OSA Secondary to COPD Claim
Helpful evidence may include:
- A sleep study confirming obstructive sleep apnea.
- CPAP, BiPAP, APAP, oxygen, or oral appliance records.
- Proof that COPD or another respiratory condition is service-connected.
- Pulmonary function tests.
- Pulmonary clinic notes.
- Records documenting chronic bronchitis, emphysema, asthma, restrictive lung disease, hypoxemia, or respiratory failure.
- Oxygen saturation data.
- Emergency room visits or hospitalizations for respiratory exacerbations.
- Medication history, including inhalers, steroids, oxygen therapy, or respiratory treatments.
- Weight history.
- Records documenting shortness of breath, fatigue, reduced activity, exercise intolerance, or inability to tolerate exertion.
- Lay statements from a spouse, partner, family member, or roommate describing snoring, gasping, choking, witnessed apneas, coughing at night, daytime sleepiness, fatigue, or PAP intolerance.
- Prior VA denial letters.
- C&P exam opinions.
The more complete the records, the easier it is to identify the strongest medically supportable theory.
Do I Need a Nexus Letter for OSA Secondary to COPD?
Not every claim requires a private nexus letter. However, many veterans seek one when the claim involves a complex secondary relationship or when VA has already denied the claim.
A nexus letter may be helpful if:
- You have a confirmed diagnosis of obstructive sleep apnea.
- You are service-connected for COPD or another respiratory condition.
- Your sleep apnea was diagnosed after service.
- The VA denied your OSA claim.
- The VA stated that COPD and OSA are unrelated.
- The VA blamed obesity without discussing respiratory limitations.
- The VA failed to address aggravation.
- The VA ignored COPD–OSA overlap syndrome.
- The VA did not consider steroid-related weight gain or reduced activity.
- The VA did not discuss nocturnal oxygen desaturation or PAP treatment complexity.
While no nexus letter can guarantee approval, a thorough physician-written opinion can help strengthen the medical evidence supporting the claim.
How Dr. Allen Addresses Common VA Objections
When preparing a nexus letter for OSA secondary to bronchitis, emphysema, or COPD, Dr. Allen looks closely at the reasoning VA commonly uses to deny these claims.
- If the VA says COPD and OSA are separate conditions, she explains whether overlap syndrome or respiratory interaction is medically relevant.
- If the VA says COPD cannot cause upper airway obstruction, she evaluates whether aggravation, oxygenation burden, reduced activity, medication effects, or intermediate-step obesity are better supported theories.
- If the VA blames obesity, she reviews whether COPD contributed to weight gain through fatigue, shortness of breath, reduced activity, repeated exacerbations, or steroid exposure.
- If the VA ignores aggravation, she explains whether COPD worsened OSA symptoms, treatment complexity, oxygen desaturation, or functional impairment beyond natural progression.
- If the VA relies on a generic opinion, she provides an individualized explanation based on the veteran’s actual records.
This type of analysis can be especially important after a denial, because a rebuttal nexus letter should address the specific weaknesses in the VA examiner’s rationale.
Why Choose Dr. Jessica Allen for Your Sleep Apnea Nexus Letter?
When filing a VA claim for sleep apnea secondary to COPD, a veteran often needs more than a brief statement or generic letter. A strong nexus letter should address both the medical evidence and the VA claim standard in a clear, organized, and medically supportable way. This is especially important because claims involving obstructive sleep apnea secondary to COPD are often medically complex and may require discussion of causation, aggravation, respiratory impairment, sleep study findings, oxygenation issues, PAP therapy, medication effects, weight history, and prior VA denial rationales.
Dr. Jessica Allen is a physician and psychiatrist with experience evaluating veterans, reviewing VA medical evidence, and preparing detailed medical nexus opinions. As a former VA Compensation & Pension examiner, she understands how VA examiners commonly analyze disability claims, how denial rationales are often written, and what a well-supported medical opinion should address. This background allows her to evaluate the veteran’s claim from both a clinical and VA-relevant perspective.
A claim for obstructive sleep apnea secondary to COPD may involve several important medical issues, including pulmonary impairment, nocturnal oxygen desaturation, CPAP, BiPAP, APAP, or oxygen treatment, COPD–OSA overlap syndrome, steroid exposure, weight gain or obesity as an intermediate step, aggravation, and the reasoning used in prior VA decisions or C&P examinations. Dr. Allen reviews these issues carefully and explains how they apply to the veteran’s specific medical history rather than relying on broad or unsupported conclusions.
Dr. Allen’s nexus letters are physician-written, evidence-based, and tailored to the veteran’s records. They are designed to address the specific claim theory involved, whether that includes causation, aggravation, COPD–OSA overlap syndrome, obesity as an intermediate step, or rebuttal of a prior VA denial. Her opinions are written in professional medical-legal language, supported by relevant medical literature when appropriate, and organized in a format suitable for submission as part of a VA disability claim.
Dr. Allen provides serious, medically reasoned opinions designed to help support a veteran’s claim when the evidence allows it. Her goal is to provide a clear explanation of the medical relationship between the veteran’s service-connected respiratory condition and obstructive sleep apnea, using the veteran’s actual records, symptoms, treatment history, and claim evidence.