VA Denied Sleep Apnea Because of Obesity?

Ask the Question the VA May Have Missed: Who Caused the Weight Gain?
Many veterans are denied service connection for obstructive sleep apnea because the VA says the condition is “due to obesity,” “due to weight gain,” or “related to body habitus.”
But that explanation may stop too soon.
The real question is not always whether obesity contributed to obstructive sleep apnea. In many cases, the more important question is:
If the VA blamed obesity, who or what caused the veteran to gain weight?
For many veterans, weight gain did not happen in isolation. It developed after service-connected PTSD, depression, anxiety, chronic pain, orthopedic injuries, medication side effects, fatigue, insomnia, or reduced activity began affecting daily life.
At Brightview Psychiatry Solutions, Dr. Jessica Allen provides independent medical nexus letters for veterans pursuing VA disability claims for obstructive sleep apnea secondary to obesity or weight gain as an intermediate step.
When medically supportable, Dr. Allen explains how a veteran’s service-connected condition may have contributed to weight gain, and how that weight gain may have contributed to the development or worsening of obstructive sleep apnea.
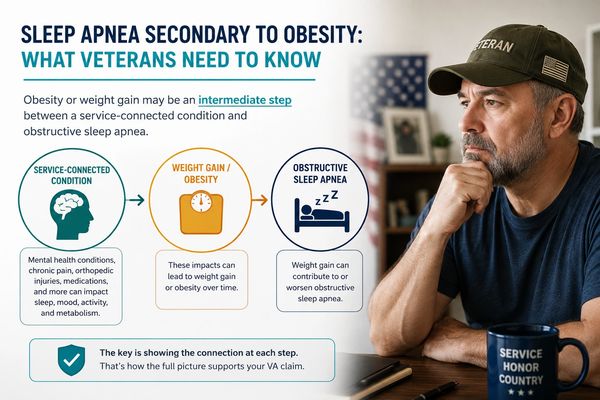
Sleep Apnea Secondary to Obesity: What Veterans Need to Know
Obesity is generally not treated as a stand-alone VA disability. However, obesity or weight gain may still matter in a VA claim if it served as an intermediate step between a service-connected condition and obstructive sleep apnea.
That means the claim is not simply:
“I have obesity, so I should be service-connected.”
Instead, the claim is:
“My service-connected condition contributed to weight gain, and that weight gain contributed to my obstructive sleep apnea.”
This distinction is important because many VA denials focus only on obesity as a risk factor for sleep apnea. They may fail to explain why the veteran gained weight in the first place.
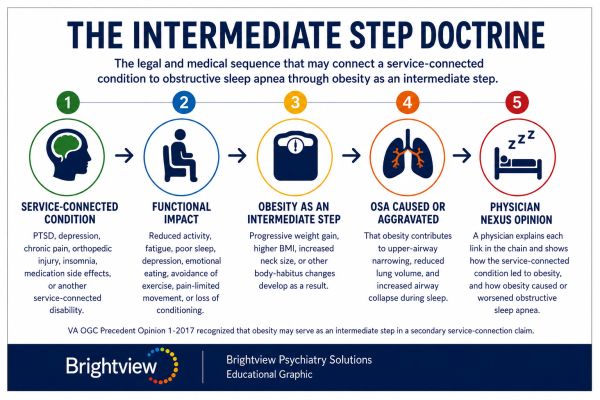
The Intermediate Step Doctrine: How Obesity Can Connect a Service-Connected Condition to Sleep Apnea
The VA generally does not treat obesity itself as a separately ratable disability. However, the VA Office of General Counsel has recognized that obesity may serve as an “intermediate step” between a veteran’s service-connected disability and another condition, such as obstructive sleep apnea.
In practical terms, this means that a veteran may be able to support service connection for obstructive sleep apnea when the medical evidence shows the following chain:
Step 1: A service-connected condition caused functional changes.
Examples may include PTSD, depression, anxiety, chronic pain, orthopedic injuries, insomnia, migraines, medication side effects, or another service-connected disability that affects sleep, activity level, metabolism, motivation, pain tolerance, or daily functioning.
Step 2: Those functional changes caused or contributed to weight gain or obesity.
This may occur through reduced physical activity, pain-limited movement, poor sleep, fatigue, emotional eating, medication-related weight gain, avoidance behaviors, sedation, loss of conditioning, or reduced ability to exercise.
Step 3: The weight gain or obesity caused or aggravated obstructive sleep apnea.
Excess weight can increase the risk of upper-airway narrowing, reduced lung volume, airway collapse during sleep, and worsening sleep-disordered breathing.
When these steps are supported by the veteran’s medical history and explained in a physician-written nexus opinion, obesity may serve as the intermediate link between the service-connected condition and the veteran’s obstructive sleep apnea.
This framework helps answer an important question that VA sometimes overlooks:
Did the VA blame obesity without asking what caused the weight gain?
A strong nexus letter should do more than state that obesity is associated with sleep apnea. It should explain, in the veteran’s specific case, how the service-connected condition caused or aggravated weight gain, how that weight gain contributed to obstructive sleep apnea, and why the medical evidence supports the connection under VA’s secondary service connection framework.
At Brightview Psychiatry Solutions, Dr. Allen evaluates each part of this chain individually, including the veteran’s service-connected conditions, functional limitations, weight history, sleep apnea diagnosis, treatment records, and relevant medical literature.
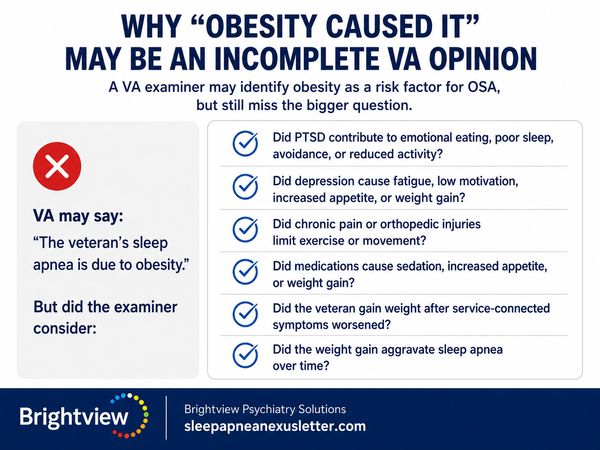
Why “Obesity Caused It” May Be an Incomplete VA Opinion
VA examiners often state that a veteran’s obstructive sleep apnea is due to obesity. That may be partly true, but it may still be incomplete.
A medical opinion can identify obesity as a risk factor and still miss the larger issue.
For example, a VA examiner may say:
“The veteran’s sleep apnea is more likely due to obesity.”
But the examiner may fail to ask:
- Did PTSD contribute to emotional eating, poor sleep, avoidance, or reduced activity?
- Did depression cause fatigue, low motivation, increased appetite, or weight gain?
- Did chronic pain make exercise difficult?
- Did orthopedic injuries limit walking, running, standing, or lifting?
- Did medications cause sedation, increased appetite, or weight gain?
- Did the veteran gain weight after service-connected symptoms worsened?
- Did the weight gain aggravate sleep apnea over time?
If those questions are not addressed, the opinion may not fully analyze the veteran’s medical history.

If Your OSA Claim Was Denied Due to Obesity
When the VA Cites Obesity as an Independent Cause — And What to Do
The VA frequently denies sleep apnea claims by concluding that obesity is the independent cause of the veteran's OSA and therefore that no service connection exists. This type of denial often reflects an incomplete analysis — specifically, a failure to consider whether the veteran's obesity itself is connected to a service-connected condition.
When the VA issues this type of denial, the veteran may file a Supplemental Claim within one year of the rating decision and submit a physician-written nexus letter as new and relevant evidence. The letter should directly address the denial reasoning and explain why the intermediate step analysis supports service connection despite obesity being a contributing factor.
A nexus letter that simply reasserts the connection without addressing the VA's specific reasoning is unlikely to change the outcome. The opinion must engage with what VA said, explain why the obesity is not an independent cause but rather a consequence of the service-connected condition, and provide the individualized medical reasoning that was missing from the original record.
Because the one-year window from the date of the denial can affect the veteran's effective date and back pay, veterans who have received this type of denial should not delay in seeking a physician opinion.

What Is an OSA Nexus Letter for Obesity?
An OSA nexus letter is a medical opinion that explains whether a veteran’s obstructive sleep apnea is at least as likely as not related to service or to an already service-connected condition.
For sleep apnea secondary to obesity or weight gain, a nexus letter should answer three core questions:
1. Did the veteran’s service-connected condition contribute to weight gain?
This may involve PTSD, depression, anxiety, chronic pain, orthopedic injuries, medications, fatigue, insomnia, or reduced activity.
2. Did the weight gain contribute to obstructive sleep apnea?
Weight gain can increase the risk or severity of OSA by worsening upper-airway narrowing and airway collapse during sleep.
3. Would the veteran’s OSA have developed, or become as severe, without the service-connected condition and resulting weight gain?
This is where the intermediate-step theory becomes important.
A strong nexus letter does not simply say obesity is associated with sleep apnea. It explains the veteran’s specific medical chain.
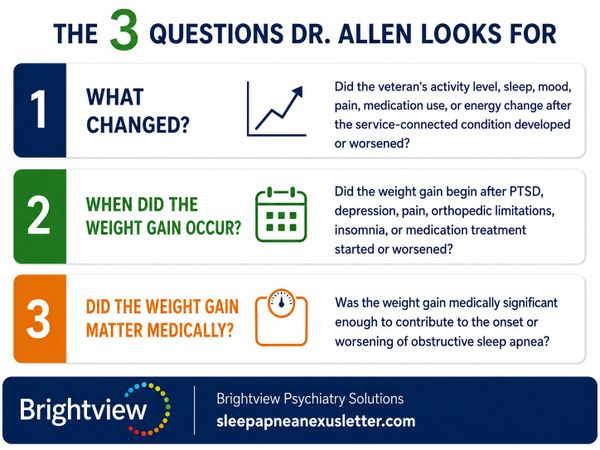
The Three Questions Dr. Allen Looks For
When reviewing a possible sleep apnea nexus letter involving obesity or weight gain, Dr. Allen looks for a medically supportable timeline.
1. What changed?
Did the veteran’s activity level, sleep, mood, pain, medication use, or energy change after the service-connected condition developed or worsened?
For example, a veteran with chronic back pain may no longer be able to exercise. A veteran with PTSD may avoid gyms or public spaces. A veteran with depression may lose motivation and gain weight gradually over time.
2. When did the weight gain occur?
Timing matters.
If weight gain occurred after service-connected PTSD, depression, chronic pain, orthopedic injury, insomnia, or medication treatment began, that timeline may help support the intermediate-step theory.
3. Did the weight gain matter medically?
Not every pound of weight gain causes sleep apnea. The question is whether the veteran’s weight gain was medically meaningful enough to contribute to the development or worsening of obstructive sleep apnea.
Dr. Allen reviews the veteran’s records to determine whether this theory is medically supportable.
What Compensation Could Look Like
The Financial Impact of Getting OSA Service-Connected
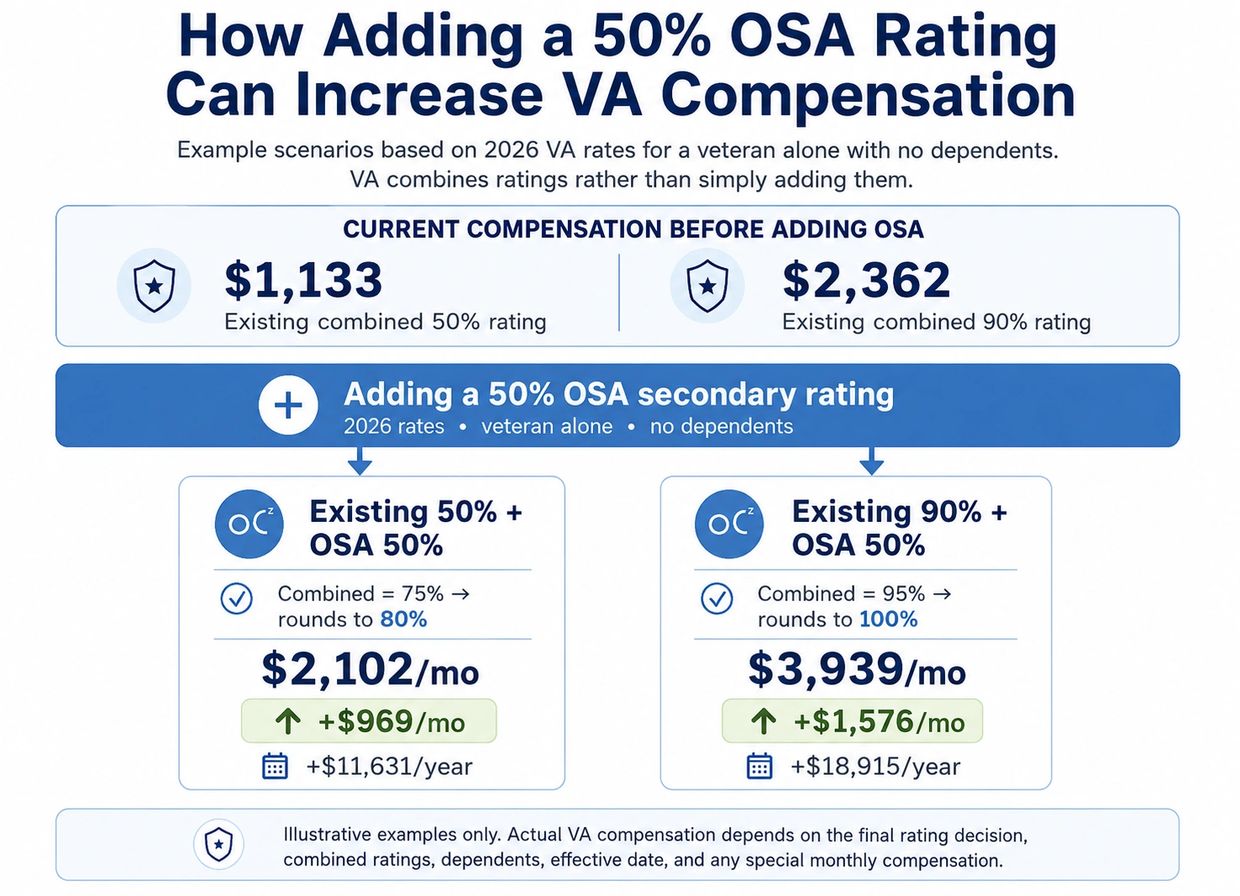
Most veterans with obstructive sleep apnea who require a CPAP machine receive a 50% VA disability rating. The financial impact of adding a 50% OSA rating to existing service-connected conditions can be substantial, particularly for veterans who are already rated at 30%, 50%, or 70% for conditions like PTSD, musculoskeletal injuries, or other disabilities.
The chart above shows estimated monthly compensation increases using 2026 VA rates for a veteran with no dependents. Veterans with spouses or dependents will receive higher amounts. Schedule a free consultation to discuss what service connection for sleep apnea could mean for your specific rating.
2026 VA rates effective December 1, 2025. Veteran alone, no dependents. Combined ratings calculated per 38 CFR 4.25. Rounded to nearest 10% per VA policy.
Learn More
We understand the financial commitment associated with securing a nexus letter. Discuss your case with Dr. Allen to determine if you have a strong case.
Common Service-Connected Conditions That May Lead to Obesity

Many different service-connected conditions may serve as the first link in an obesity-as-an-intermediate-step claim. The key question is not simply whether the veteran has obesity or obstructive sleep apnea. The key question is whether the veteran’s service-connected condition caused or contributed to weight gain in a medically supportable way, and whether that weight gain then caused or aggravated obstructive sleep apnea.
Common starting points include the following.
Musculoskeletal Injuries and Chronic Pain
Service-connected back injuries, neck conditions, radiculopathy, knee injuries, hip conditions, ankle injuries, foot conditions, shoulder injuries, and other orthopedic disabilities may limit a veteran’s ability to engage in physical activity.
A veteran who was previously able to run, lift weights, exercise regularly, or perform physically demanding work may no longer be able to maintain the same level of activity after a service-connected injury. Even when some activity remains possible, the intensity, frequency, and consistency of exercise may be significantly reduced.
Over time, reduced activity, pain-limited movement, deconditioning, and avoidance of painful activity may contribute to progressive weight gain. If that weight gain later contributes to obstructive sleep apnea, the orthopedic or chronic pain condition may be medically relevant as the first link in the intermediate-step chain.
PTSD and Mental Health Conditions
Service-connected PTSD, depression, anxiety, and other mental health conditions may contribute to weight gain through several pathways. These may include poor sleep, nightmares, hypervigilance, fatigue, low motivation, social withdrawal, emotional eating, alcohol use, avoidance of gyms or crowded spaces, and reduced physical activity.
Some veterans with PTSD avoid public spaces, outdoor activity, or structured exercise because those environments trigger anxiety, irritability, panic symptoms, or hypervigilance. Depression may make it harder to maintain daily routines, prepare healthy meals, exercise consistently, or stay socially engaged. Anxiety may worsen insomnia and fatigue, which can further reduce activity levels.
When a service-connected mental health condition contributes to weight gain, and that weight gain contributes to obstructive sleep apnea, the mental health condition may be part of the medical chain connecting the veteran’s service-connected disability to OSA.
Medication-Related Weight Gain
Medication history can be important in obesity-related sleep apnea claims. Some medications used to treat service-connected mental health symptoms, insomnia, pain, neurologic symptoms, inflammation, or muscle spasms may contribute to increased appetite, sedation, fatigue, reduced activity, metabolic changes, or weight gain.
This may include certain antidepressants, antipsychotic medications, mood stabilizers, sleep medications, pain medications, corticosteroids, and other medications depending on the veteran’s specific treatment history.
A strong nexus opinion should not rely on generic assumptions about medication side effects. It should review the veteran’s actual medication history, the timing of weight changes, the reason each medication was prescribed, and whether the medication was used to treat a service-connected condition. When supported by the records, medication-related weight gain may form part of the causal chain.
Traumatic Brain Injury
Service-connected traumatic brain injury may also be relevant in some obesity-related OSA claims. TBI can contribute to changes in sleep, activity level, mood, cognition, impulse control, fatigue, and executive functioning. In some cases, these effects may make it more difficult for a veteran to maintain consistent exercise, meal planning, sleep routines, or weight management.
When the medical records support a connection between service-connected TBI, weight gain, and obstructive sleep apnea, TBI may serve as part of the intermediate-step analysis.
Fibromyalgia and Chronic Fatigue
Service-connected fibromyalgia and chronic fatigue syndrome may significantly reduce a veteran’s tolerance for physical exertion. Veterans with these conditions may experience pain flares, post-exertional fatigue, poor sleep, reduced endurance, and difficulty maintaining consistent physical activity.
Over time, reduced activity and impaired exercise tolerance may contribute to weight gain. If that weight gain contributes to obstructive sleep apnea, fibromyalgia or chronic fatigue syndrome may be medically relevant to the nexus analysis.
Why the Specific Medical Chain Matters
A general statement that obesity is associated with sleep apnea is usually not enough. The opinion should explain the veteran’s specific medical sequence:
Service-connected condition → functional limitation or medication effect → weight gain → increased OSA risk → OSA diagnosis or worsening.
At Brightview Psychiatry Solutions, Dr. Allen reviews the veteran’s service-connected conditions, functional limitations, medication history, weight history, sleep study findings, and relevant medical literature to determine whether the obesity-as-an-intermediate-step theory is medically supportable in that veteran’s specific case.
How a Nexus Letter From Dr. Allen Can Help
What Dr. Allen Provides
Dr. Jessica Allen provides independent, records-based medical nexus letters for veterans seeking to support claims for obstructive sleep apnea secondary to obesity or weight gain as an intermediate step.
Dr. Allen may review:
- Sleep study results.
- VA rating decisions.
- VA denial letters.
- C&P examination reports.
- VA and private medical records.
- Medication history.
- Weight history and BMI trends.
- Mental health records.
- Pain and orthopedic records.
- Lay statements from the veteran, spouse, family, or others.
- Prior unfavorable VA medical opinions.
When the evidence supports the opinion, Dr. Allen explains whether it is at least as likely as not that the veteran’s service-connected condition caused or aggravated weight gain, and whether that weight gain contributed to the development or worsening of obstructive sleep apnea.
The goal is to provide VA with a clear medical explanation that addresses the question the denial may have missed:
VA blamed obesity — but what caused the weight gain?
What Makes This Type of Nexus Letter Different?
A generic nexus letter may simply state that obesity is associated with sleep apnea.
That is usually not enough.
A stronger opinion should explain the veteran’s individual medical timeline:
- What service-connected conditions does the veteran have?
- When did weight gain begin?
- Did PTSD, depression, pain, fatigue, insomnia, or medications affect the veteran’s activity level?
- Did orthopedic injuries limit exercise?
- Did the veteran gain weight after service-connected symptoms worsened?
- When was sleep apnea diagnosed?
- Did VA deny the claim by blaming obesity without analyzing the cause of the weight gain?
This veteran-specific explanation is what can make an intermediate-step opinion more persuasive.