
Nexus Letters For Sleep Apnea
Sleep Apnea Nexus Letter for OSA Secondary to PTSD
Physician-written nexus letters by Dr. Jessica Allen, M.D., psychiatrist and former VA C&P examiner.
Sleep Apnea Nexus Letters Secondary to PTSD
.png/:/cr=t:0%25,l:0%25,w:100%25,h:100%25/rs=w:600,cg:true)
What Does “Sleep Apnea Secondary to PTSD” Mean?
A secondary VA disability claim means that a current condition was caused or aggravated by an already service-connected condition. For this type of claim, PTSD is the service-connected condition, and obstructive sleep apnea is the secondary condition.
An OSA secondary to PTSD claim may be medically supportable when the evidence shows that PTSD contributed to the development or worsening of sleep apnea through factors such as chronic insomnia, fragmented sleep, nightmares, hyperarousal, psychiatric medication side effects, weight gain, reduced activity, alcohol use, or difficulty tolerating CPAP therapy.
This distinction is important because VA examiners may deny claims by stating that PTSD does not directly cause a mechanical airway obstruction. However, obstructive sleep apnea is multifactorial, and a complete medical opinion should consider whether PTSD caused, contributed to, or aggravated OSA through the veteran’s specific symptoms, treatment history, medications, weight changes, and sleep-related impairment.
Dr. Allen’s nexus letters do not rely on a generic statement that “PTSD causes sleep apnea.” Instead, they explain whether the veteran’s records support a medically reasoned connection between service-connected PTSD and obstructive sleep apnea.
.png/:/rs=w:600,cg:true,m)
Why the VA Often Denies Sleep Apnea Secondary to PTSD Claims
Many veterans are denied because a VA examiner concludes that PTSD and sleep apnea are “separate conditions” or that OSA is caused by obesity, age, anatomy, or other risk factors.
Common VA denial issues include:
- The examiner states that PTSD does not cause sleep apnea.
- The examiner blames obesity without asking whether PTSD contributed to weight gain.
- The examiner ignores aggravation.
- The examiner does not discuss medication side effects.
- The examiner overlooks insomnia, nightmares, fatigue, hyperarousal, or CPAP intolerance.
- The examiner fails to consider lay statements from a spouse, partner, or family member.
Dr. Allen’s nexus letter is designed to address these weaknesses directly. If the VA blamed obesity, she evaluates whether PTSD contributed to the veteran’s weight gain. If the VA ignored aggravation, she explains whether PTSD worsened OSA or made treatment less effective. If the VA relied on a generic opinion, she provides an individualized medical analysis based on the veteran’s records.
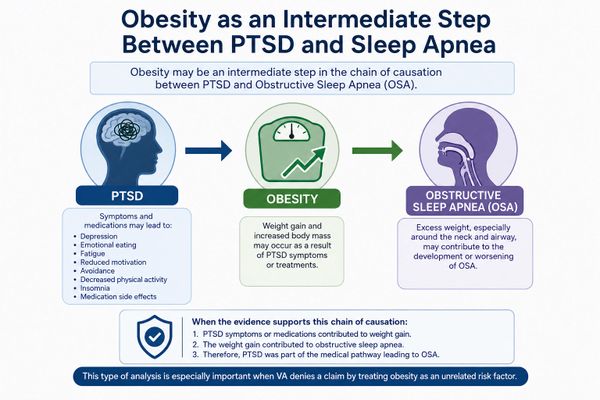
Obesity as an Intermediate Step Between PTSD and Sleep Apnea
Obesity is one of the most common reasons VA denies sleep apnea claims. However, obesity does not automatically defeat a claim.
In some cases, obesity may be an intermediate step between PTSD and obstructive sleep apnea. PTSD may contribute to weight gain through depression, emotional eating, fatigue, reduced motivation, avoidance, decreased physical activity, insomnia, and medication side effects. That weight gain may then contribute to the development or worsening of OSA.
When the evidence supports this theory, Dr. Allen explains the chain of causation:
- PTSD symptoms or medications contributed to weight gain.
- The weight gain contributed to obstructive sleep apnea.
- Therefore, PTSD was part of the medical pathway leading to OSA.
This type of analysis is especially important when VA denies a claim by treating obesity as an unrelated risk factor.
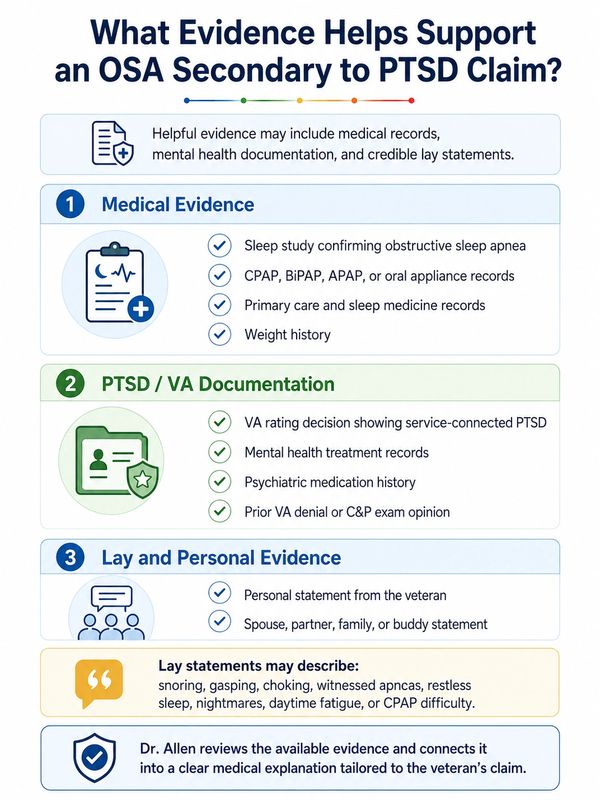
What Evidence Helps Support an OSA Secondary to PTSD Claim?
Helpful evidence may include:
- Sleep study confirming obstructive sleep apnea.
- CPAP, BiPAP, APAP, or oral appliance records.
- VA rating decision showing service-connected PTSD.
- Mental health treatment records.
- Psychiatric medication history.
- Weight history.
- Primary care and sleep medicine records.
- Prior VA denial or C&P exam opinion.
- Personal statement from the veteran.
- Spouse, partner, family, or buddy statement.
Lay statements may be useful when they describe snoring, gasping, choking, witnessed apneas, restless sleep, nightmares, daytime fatigue, or CPAP difficulty.
Dr. Allen reviews the available evidence and connects it into a clear medical explanation tailored to the veteran’s claim.
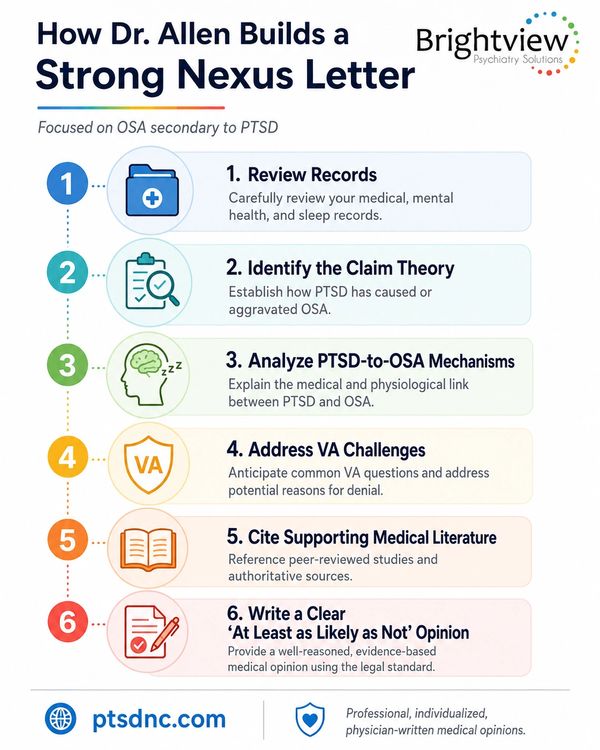
What Is a Nexus Letter for Sleep Apnea Secondary to PTSD?
A nexus letter is a medical opinion explaining the relationship between a diagnosed disability and a service-connected condition.
For OSA secondary to PTSD, Dr. Allen’s nexus letter addresses whether the veteran’s obstructive sleep apnea is at least as likely as not proximately due to, the result of, and/or aggravated by service-connected PTSD.
Her letter may include:
- Review of relevant medical records.
- Summary of PTSD history and symptoms.
- Summary of sleep apnea diagnosis and treatment.
- Discussion of sleep study findings.
- Analysis of PTSD-related sleep disruption, fatigue, weight changes, and CPAP intolerance.
- Review of psychiatric medications and their possible impact on OSA.
- Discussion of obesity as an intermediate step, when applicable.
- Analysis of causation and aggravation.
- Response to prior VA denial reasoning, when applicable.
- Citation to relevant medical literature.
- Clear medical opinion using VA-relevant language.
A strong nexus letter should explain not only the conclusion, but the reasoning behind it.
Current VA Disability Ratings for Sleep Apnea
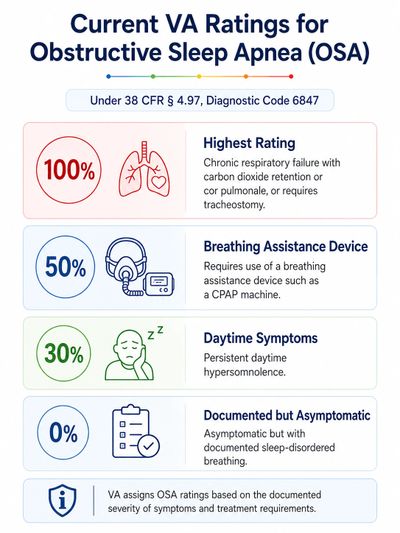
Has the VA Changed the Ratings for Sleep Apnea?
As of June 2026, the VA has not implemented a change to the rating criteria for obstructive sleep apnea. OSA continues to be rated under 38 C.F.R. § 4.97, Diagnostic Code 6847, with ratings of 0%, 30%, 50%, or 100% depending on the documented severity of symptoms and treatment requirements.
Why a Sleep Apnea Rating Can Matter Financially

How Service Connection for Sleep Apnea May Increase VA Compensation
If VA grants service connection for obstructive sleep apnea, the financial impact can be significant. In many cases, veterans who require a CPAP machine may qualify for a 50% sleep apnea rating, which can substantially increase overall monthly compensation. Because VA uses a combined ratings formula, disability percentages are not simply added together. The examples below show how adding a 50% OSA rating to common PTSD rating scenarios may affect compensation based on 2026 VA rates for a veteran alone with no dependents. Actual compensation depends on the final rating decision, combined ratings, dependents, and effective date.