Claiming Sleep Apnea Secondary to Rhinitis
Sleep Apnea Secondary to Rhinitis: VA Disability Nexus Letters for Veterans
Many veterans developed allergic or chronic rhinitis during military service — from exposure to sand, dust, burn pits, chemical irritants, or environmental allergens encountered during deployment. Chronic nasal inflammation and congestion do more than cause day-to-day discomfort. Over time, they can directly contribute to the development or worsening of obstructive sleep apnea.
If you are already service-connected for allergic or chronic rhinitis and have been diagnosed with obstructive sleep apnea, you may be able to file a claim for sleep apnea secondary to rhinitis. As with any secondary claim, the VA generally requires medical evidence explaining how the service-connected rhinitis caused, contributed to, or aggravated the sleep apnea — not simply that both conditions are present.
At Brightview Psychiatry Solutions, our physicians provide independent medical nexus letters for veterans pursuing sleep apnea claims secondary to rhinitis, sinusitis, obesity, PTSD, and other conditions connected to military service.
Quick Answer
Yes, obstructive sleep apnea may be claimed as secondary to service-connected allergic, chronic, or vasomotor rhinitis when the evidence shows that chronic nasal obstruction, congestion, mouth breathing, increased airway resistance, or CPAP intolerance caused or aggravated the veteran’s OSA. The strongest claims usually include a sleep study, proof of service-connected rhinitis, documented nasal symptoms, and a medical nexus opinion explaining the relationship.
Can Sleep Apnea Be Secondary to Rhinitis?
What is the Connection Between Rhinitis and OSA?
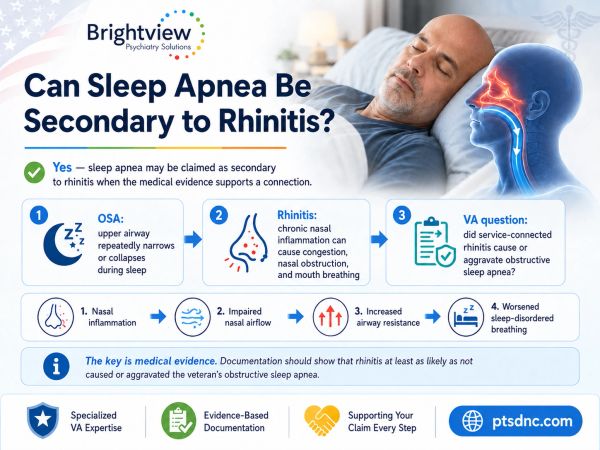
Sleep apnea may be claimed as secondary to rhinitis when the medical evidence supports a connection.
Rhinitis is inflammation of the nasal passages, causing nasal congestion, swelling, postnasal drip, and obstructed airflow through the nose. It may be allergic, caused by an immune response to pollen, dust, mold, or other allergens, or non-allergic, caused by irritants such as smoke, chemical exposure, or environmental pollutants commonly encountered during deployment.
When the nasal passages are chronically inflamed or obstructed, airflow through the nose is restricted. This forces mouth breathing during sleep, which can destabilize the upper airway and increase the likelihood of obstructive events. Chronic nasal obstruction is recognized in the medical literature as a contributing factor to obstructive sleep apnea, particularly when the condition is long-standing and untreated.
This mechanism is closely related to the airway obstruction pathway seen in sleep apnea secondary to sinusitis claims, and veterans with both conditions may have overlapping or combined theories of entitlement.

VA Secondary Service Connection for Sleep Apnea Due to Rhinitis: What the VA Requires
To establish sleep apnea secondary to rhinitis, veterans generally need three types of evidence.
1. A Current Diagnosis of Obstructive Sleep Apnea
Typically confirmed through a sleep study, with documentation of severity and any prescribed breathing assistance device such as a CPAP, APAP, BiPAP, or oral appliance.
2. A Service-Connected Rhinitis Diagnosis
The veteran should already be service-connected for allergic or chronic rhinitis, rated under 38 CFR § 4.97, Diagnostic Code 6522, or be pursuing that service connection concurrently.
3. A Medical Nexus Between Rhinitis and Sleep Apnea
The nexus letter should explain why the veteran's sleep apnea is at least as likely as not proximately due to, the result of, or aggravated by the service-connected rhinitis — addressing the veteran's specific nasal obstruction findings, symptom history, and how those findings relate to the sleep apnea diagnosis.

Causation vs. Aggravation: There Are Two Ways to Argue This Claim
There are two major ways to argue sleep apnea secondary to rhinitis. After reviewing your medical history, Dr. Allen will be able to determine which approach to take in your nexus letter:
Causation
Causation means the service-connected rhinitis directly contributed to the development of obstructive sleep apnea — for example, when chronic nasal obstruction predates the OSA diagnosis and no other major risk factor explains the onset.
Aggravation
Aggravation means the rhinitis made an existing or developing sleep apnea worse, even when other factors are also present. This may be the stronger theory when a veteran has other risk factors such as obesity or anatomy, but the rhinitis-related nasal obstruction is shown to independently worsen the severity or treatment-resistance of the OSA.
A thorough nexus letter should evaluate both theories and identify which is best supported by the veteran's specific medical history.
How Service-Connection for OSA Impacts Your Monthly Pay
How a 50% OSA Rating May Increase Monthly VA Compensation
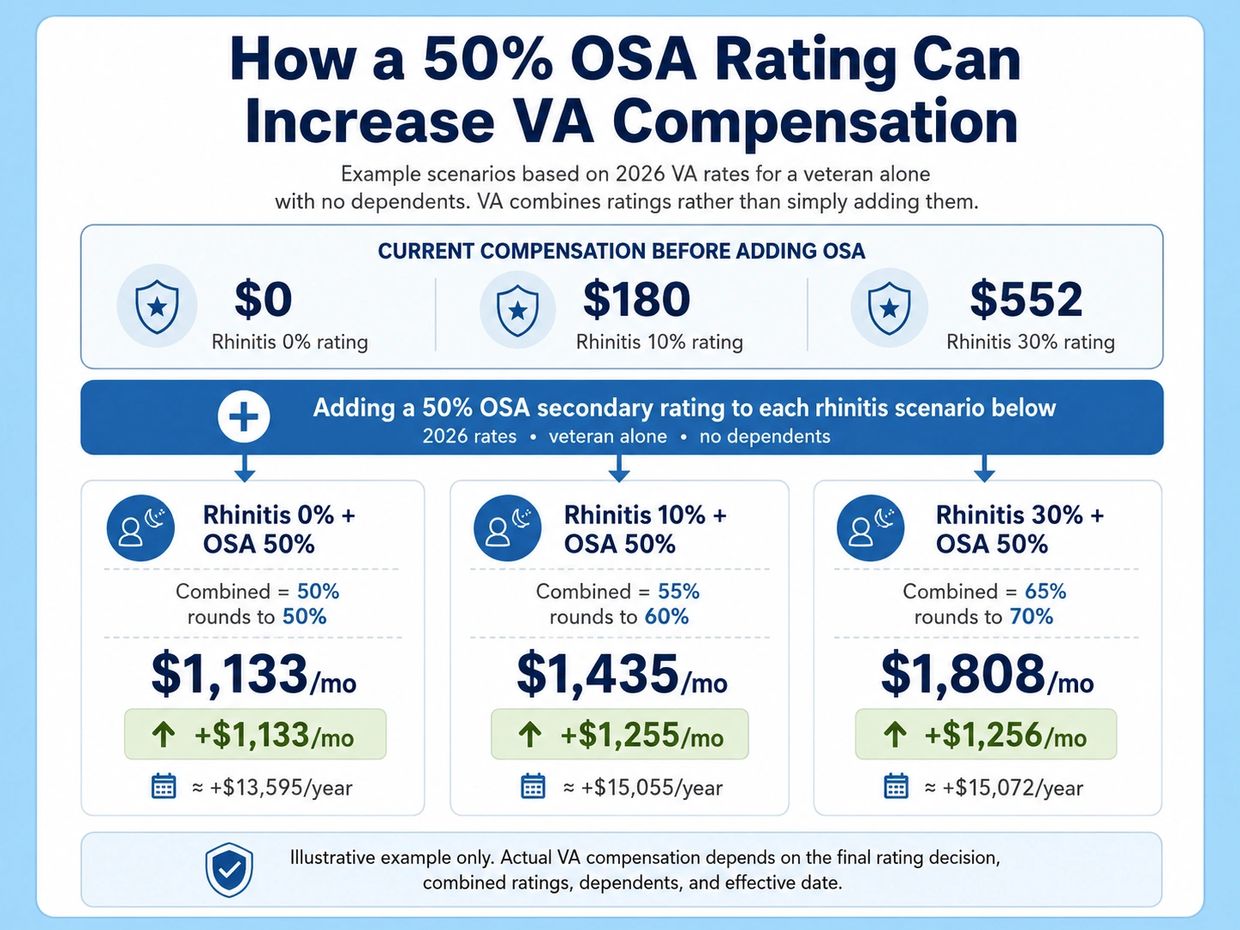
Veterans with chronic rhinitis are commonly assigned VA ratings of 0%, 10%, or 30%, depending on the severity of nasal obstruction and whether nasal polyps are present. When obstructive sleep apnea is claimed as secondary to service-connected rhinitis, a favorable VA decision assigning a 50% OSA rating may significantly increase monthly compensation.
It is important to understand that VA does not simply add disability ratings together. Instead, the VA uses its combined ratings formula, which means a 30% rating combined with a 50% rating does not equal 80%; it combines to 65%, which rounds to 70%. The graphic below shows how adding a 50% OSA rating may affect compensation in common rhinitis-rating scenarios for a veteran with no dependents.
These figures are provided for educational purposes only. Actual compensation depends on the veteran’s final combined rating, effective date, dependent status, and the outcome of VA’s review.
Service Connection for Sleep Apnea Denied, What to Do Next?
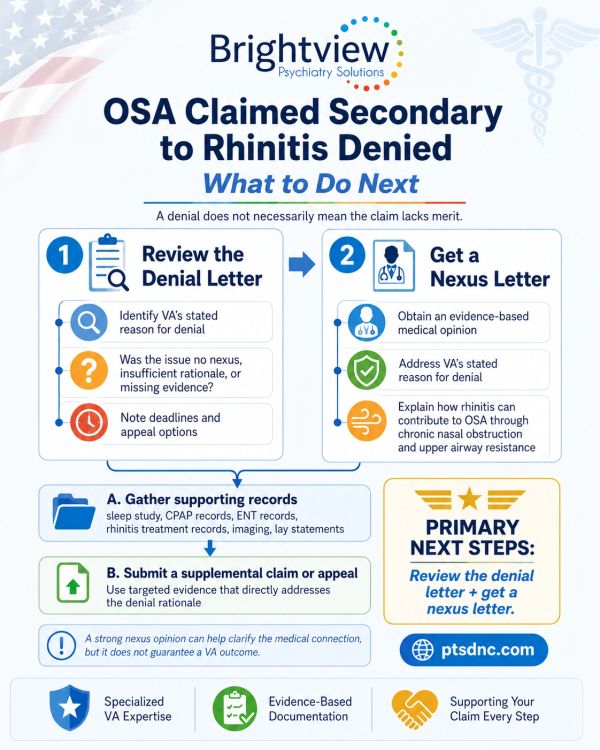
Common Reasons the VA Denies Sleep Apnea Secondary to Rhinitis Claims
Common reasons for denial include:
- The VA acknowledges both diagnoses but finds no medical nexus
- The VA attributes the OSA to obesity, age, or anatomy instead
- The examiner concludes rhinitis and OSA are unrelated conditions
- The nexus opinion submitted is too brief or conclusory
- The claim does not separately address aggravation
If your claim has been denied, you generally have one year from the date of the rating decision to file a Supplemental Claim with new and relevant evidence and preserve your original effective date. A physician-written nexus letter that directly addresses the VA's denial reasoning can serve as that new evidence. For more on this process, see our guide to denied OSA claims.
A nexus letter from Dr. Allen can be essential in these cases. A nexus letter can serve as new and relevant evidence for a Supplemental Claim.
Supporting Evidence For Sleep Apnea Secondary to Rhinitis
Sleep Apnea Evidence
- Sleep study results
- CPAP, APAP, BiPAP, or oral appliance prescription
- PAP compliance reports
- Reports of snoring, choking, gasping, or witnessed apneas
Rhinitis Evidence
- VA rating decision showing rhinitis is service-connected
- ENT or allergy treatment records
- Documentation of nasal obstruction findings (e.g., septal deviation, turbinate hypertrophy, polyps)
- Records of chronic congestion, postnasal drip, or recurring sinus symptoms
- History of deployment-related environmental or burn pit exposure, if applicable
Lay Statements
A spouse or family member describing chronic congestion, mouth breathing, snoring, or witnessed breathing pauses can help corroborate the medical record. Learn how a spouse's statement can support your claim →
How A Nexus Letter from Dr. Allen Can Help
Why Dr. Allen Is Especially Qualified to Write This Nexus Letter?
A persuasive nexus letter for obstructive sleep apnea secondary to chronic rhinitis requires more than a general medical statement that nasal obstruction and sleep apnea can be related. It requires a physician who can explain the specific medical reasoning connecting chronic nasal inflammation, congestion, and impaired nasal airflow to sleep-disordered breathing in the individual veteran’s case.
Dr. Jessica Allen is a physician and psychiatrist with extensive experience writing medical nexus opinions for veterans seeking VA disability benefits. Her work focuses on carefully analyzing the veteran’s medical records, service-connected conditions, symptom history, sleep study findings, treatment course, and VA rating history to determine whether the evidence supports a medically reasoned opinion for service connection.
Dr. Allen is also a former VA Compensation and Pension examiner. This experience gives her direct insight into how VA disability claims are evaluated, how medical opinions are reviewed, and why many nexus letters fail when they rely on vague conclusions instead of clear medical rationale. She understands that a strong nexus letter must do more than state that obstructive sleep apnea and rhinitis coexist. It must explain why the veteran’s chronic rhinitis at least as likely as not caused, contributed to, or aggravated the obstructive sleep apnea.
In sleep apnea claims secondary to rhinitis, Dr. Allen evaluates the full medical picture, including ENT records, documented nasal obstruction, allergic or non-allergic rhinitis symptoms, use of nasal sprays or allergy medications, sleep study results, CPAP tolerance, mouth breathing, snoring, fragmented sleep, and any evidence that nasal congestion worsens nighttime breathing. She then connects those findings to the relevant medical principles, including increased nasal airway resistance, upper-airway collapsibility, sleep fragmentation, reduced CPAP effectiveness, and worsening nocturnal oxygenation.
This individualized approach is especially important because VA examiners may deny these claims by stating, in broad terms, that rhinitis does not directly cause sleep apnea. Dr. Allen addresses that issue directly by explaining that obstructive sleep apnea is often multifactorial and that chronic rhinitis may still be a medically significant contributing or aggravating factor, even when other risk factors are present.
Dr. Allen’s role is to provide a detailed, evidence-based, VA-relevant medical opinion that applies the medical literature and clinical reasoning to the veteran’s specific facts. Her nexus letters are designed to clearly explain the connection between the veteran’s service-connected rhinitis and obstructive sleep apnea in language that is medically sound, individualized, and relevant to VA adjudication.
